
What Drug Was Worth More Than Half a Billion Dollars to Advertise Directly to Consumers?
We, as taxpayers and the people who purchase health insurance, are paying for advertised drugs. Therefore, we should have the right to demand restrictions on promoting the products we pay for.

A beautiful young woman is shown dancing at a party. She is wearing a flowing, low cut bright blue dress with exposed shoulders and hair pinned up showing as much skin as possible. The narrator says “…so you can show up with clearer skin and show it off.” Zoom to a closeup of her upper back and neck revealing an ugly, discolored lesion while we hear “With Skyrizi, you can take that next step with 90% clearer skin.”
In 2023, the largest pharma direct-to-consumer (DTC) advertising spend was for Skyrizi. (From now on I will be referring to Skyrizi by its generic name, risankizumab. We’ve probably all heard the word Skyrizi enough by now.) An eye-popping $579.7 million was invested in promoting risankizumab to the 2 million Americans who have moderate to severe plaque psoriasis in the US. About $290 per potential patient. Risankizumab is priced at $288,000 per patient per year (Table). This ad spend suggests that risankizumab brings in enough money to be worth it and contribute to ABBVie’s $1.56 billion profit in the 3rd quarter of 2024.
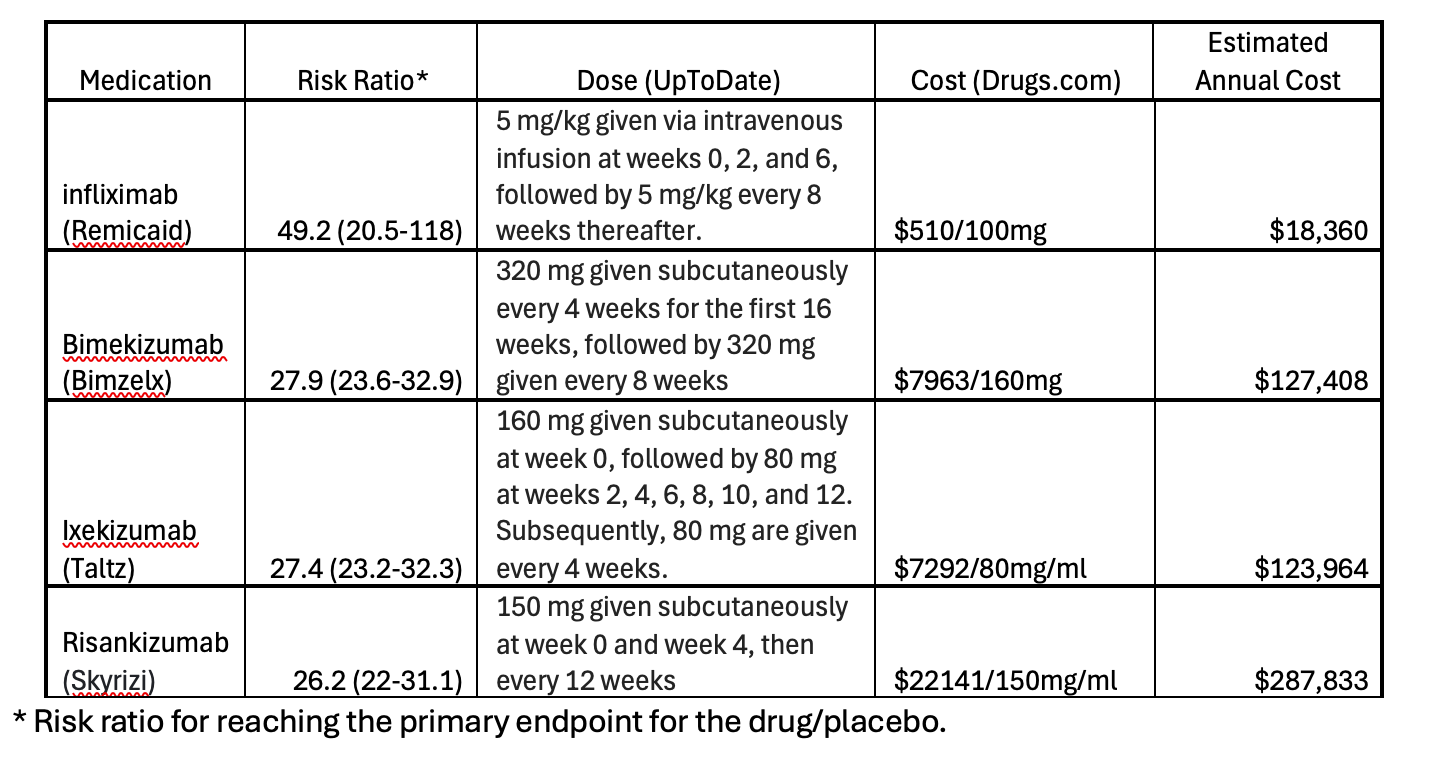
Table. Drugs for the treatment of moderate to severe plaque psoriasis. Derived from a 2023 Cochrane review of psoriasis treatments. The medications listed in this table have high certainty evidence for efficacy relative to placebo.
The risankizumab ad is misleading. It shows a psoriatic lesion involving less than 1% of body surface area (BSA).1 Drugs like risankizumab are only indicated for moderate (3-10% BSA) or severe (>10% BSA) plaque psoriasis. Viewers of the ad might believe this drug can be used to treat small, isolated lesions. They will be influenced by the visuals and are not likely to understand that risankizumab should only be used for more severe disease than is shown in the ad.
The ad will motivate patients to ask their clinicians to consider prescribing risankizumab. If the drug is not indicated for that patient’s disease, the physician will have to explain the nuances of when to use, or not use, it. They will also need to explain the very high cost of the drug, a cost that is not shown in the ad. Even if indicated, based on a 2023 Cochrane review, risankizumab is the least effective but most expensive of similar drugs used for psoriasis treatment.
All this puts the clinician in a tough spot. Explaining to a patient that something they want is not indicated can be the hardest and most time-consuming part of a clinical encounter. In today’s 15-minute encounters, this is difficult to do. It is easier for the clinician to simply prescribe the medication and move on.
Stating that risankizumab results in 90% clearer skin is misleading. True, 90% reduction in lesion surface area is the primary endpoint for psoriasis drug trials. But this endpoint was not achieved in 25% of patients receiving risankizumab in clinical trials. That about ¼ of patients treated with risankizumab will not have the anticipated clinical response is not shown in the ad. At nearly $300,000 per year, a lot of money will be spent on patients who try risankizumab but have a suboptimal response.
A patient may see the ad and decide they want to try the drug. The ad states that patients may pay as little as $5 per dose, 4 times per year. The Syrrizi.com website is listed in the TV ad as a place to go to get more information about the drug and its pricing. The price on the website is even better: $0 per dose. Who could blame a patient for believing the drug doesn’t cost much. If it did, why give it for free? But it is not free. Rather it is one of the most expensive psoriasis treatments available. Who pays? All of us. Either via medical insurance premiums or taxes we pay that are used to support Medicare or Medicaid. Because we, as a society, and not the individual patient is paying for these products, we should have some say in how they are used or promoted.
Pharma advertisers may claim a right to free speech in running DTC ads. But those who are paying for the purchase of the advertised drugs should also have the right to demand restrictions on promoting products they pay for. This situation differs from any other type of advertising where a product is presented to a viewer who decides to spend their own money to buy it. Free speech makes sense in this scenario. It does not make sense when a product is advertised to someone who decides to use the product and someone else pays for it.
One could argue that DTC advertising for prescription drugs is unethical. When advertising cars or foods, consumers can make their own decisions about how much they are willing to spend and how much risk they will assume for any product. Viewers of prescription drug ads do not know the full range of the medications’ efficacy or adverse events. If they did, there would be no need for restricting its use as prescription only. Advertising a product to someone who most likely does not know the efficacy and risk associated with its use should be considered unethical.
The incoming Trump administration is proposing to ban DTC drug advertising. The prevailing argument against this is pharma companies’ free speech rights.
The Central Hudson test outlines what is needed to ban commercial speech (in this case DTC advertising).
1) To ban advertising, the content must be misleading or promote unlawful activity
2) There needs to be a substantial government interest
3) The ban advances a substantial government interest and
4) the ban must be as narrow as possible or as least intrusive such as by adding a label to a ad or product.
One can argue that because DTC pharma ads promote the expenditure of government money through Medicare or Medicaid the government does have a substantial interest in the problem. A case could be made that often the ads are misleading. In the risankizumab ad, a person is shown who does not appear to have moderate or severe disease, misleading the viewer to believe that this drug can be used for mild disease.
If the Trump administration follows through on their expressed intentions to ban pharma DTC advertising, they should be able to justify this to the medical community based on ethical considerations. Legally, they may be able to justify DTC advertising bans because the government pays for much of the healthcare delivered in the US and pharma DTC ads inappropriately promote government expenditures.
Dr. Livingston is a Professor of Surgery at UCLA and former Deputy Editor at JAMA.
Of course, we can’t expect the ad to provide a full body skin exam, but the impression is of a single lesion.
 | A guest post by
|
As a cardiologist, I hate these ads. Almost no patient knows if they have a “moderate to severe” diagnosis. These ads are aimed at the older people watching ABC, CBS, NBC nightly news as most younger people have given up on the legacy media.
I think few issues insult a physician more than this one. The fact that big pharma advertises drugs targeting a market for those with frequently arcane diagnoses to a national audience is emblematic of the highly unethical nature of these efforts. I hope the Trump administration shuts it down and leaves New Zealand as the only country on earth that allows DTC advertising.