
What I Read This Week
Two topics I might be wrong about and two articles that didn't change my mind

I only read two articles last week (Labor Day, a wedding, having to debate, and then write an article with Vinay…). At first glance they seem very different, but they actually have quite a bit in common. Both were “suggested to me” -- one by a Sensible Medicine reader and one by a twitter-colleague. Both relate to topics I have expressed pretty strong opinions about, opinions that I fully recognize might be wrong. Although the results of both studies challenge my opinion, neither changed my mind.
I’m an avowed mammogram skeptic. Obviously, mammograms occasionally benefit people, but also do quiet harm – false positives, overdiagnosis, and radiation exposure – and I think the harm outweighs the benefit. I’m also pretty sure that mammograms are becoming less beneficial as our treatments improve. In practice, I counsel patients that mammography is the standard of care. I also individualize my recommendations, provide a variety of infographics, and respect each patient’s decision.
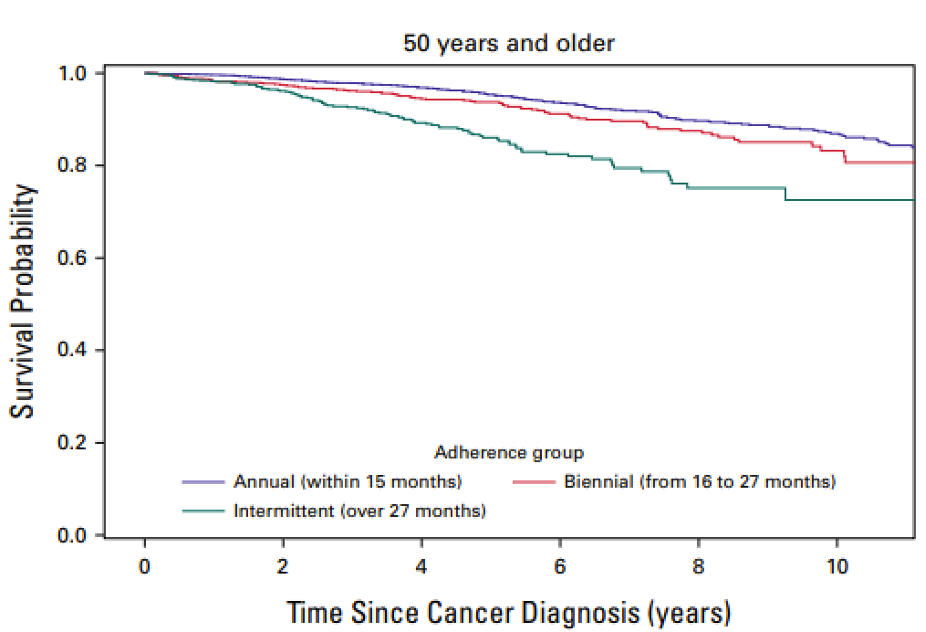
The article came out of the University of Pittsburgh and studied patients there. The researchers looked at every patient that had a mammogram between 2004 and 2019 and developed breast cancer. They categorized patients by screening interval – annual, biennial, or intermittent – and then determined the stage of the cancer at diagnosis and overall survival.
Results
Late-stage cancers were more commonly diagnosed in woman with longer screening intervals, 9%, 14%, and 19% for annual, biennial, and intermittent groups, respectively. The authors were able to show a difference in survival, adjusted for lead time bias, in the over 50 age group.
So why does this article not make me more bullish on mammography? Let me count the ways.
1. Observational data. We so desperately need RCT data for our screening tests. I understand the barriers to RCTs, but we are spending so much money on screening that might be put to better use. Not surprisingly, the people who were categorized into different groups by their screening intervals differed by a lot more than screening interval. There was adjustment for confounding but…
2. Endpoints. The purpose of screening is not to find cancer. The purpose of screening is not to find cancer earlier. The purpose of screening is not to shift the grade or stage at diagnosis. We screen to lower mortality (ideally overall mortality, not just diagnosis specific mortality). The endpoints of this observational study are inadequate. This is especially true because of the issue of lead-time bias that I am not convinced is adequately controlled for.
3. Single center. This is a single center study. We discuss in Ending Medical Reversal why we should be suspicious of single center studies. A recent article has made me even more convinced that little should be based on the results of a single center study.
I’ve come out pretty strongly against GDMT. For those less in the know, that link does a pretty good job of describing the nitty gritty of GDMT. My “opposition” to GDMT is much like my opposition to mammography. I am sure it works, I just think the cult-like (H/T Anil Makam) dedication to it is based on an overstatement of the benefit and an under-appreciation of the harms. I had read the STRONG-HF article when I wrote that “Why GDMT Bugs Me” post, but someone asked if this article made me more enthusiastic about GDMT, so I reread it. My opinion did not change.
STRONG-HF was an epic trial. In a multinational, open-label, randomized, parallel-group trial, patients aged 18–85 years, admitted to hospital with acute heart failure, were randomly assigned to either usual care or high-intensity care. High intensity care was the GDMT group. In this group, medications were up-titrated to recommended doses within 2 weeks of discharge and four scheduled outpatient visits were completed in the 2 months after discharge. The primary endpoint was 180-day readmission to hospital due to heart failure or all-cause death.
1078 patients were randomized and the study was stopped early. The results were impressive. First those assigned to GDMT were more likely to get GDMT. The differences in reaching full dose of medications were as follows: renin-angiotensin blockers, 55% vs. 2%; β blockers, 49% vs. 4%; and mineralocorticoid receptor antagonists 84% vs 46%. SGLT2s were not approved for HF at the time of this study. Clinical endpoints also differed. Heart failure readmission or all-cause death at 80 days was 15·2% in the GDMT group vs. 23·3% in the usual care group (RR 0·66 [95% CI 0·50–0·86]). There was no difference in any of the mortality endpoints. More adverse events occurred in the GDMT group (41% vs. 29%) but serious and fatal adverse events were similar.
So why does GDMT still bug me? This article doesn’t show a benefit of GDMT. It shows a benefit of close follow-up in a heart failure clinic. (It pains me to say it, but previous research has shown that cardiology follow-up is superior to primary care follow up for this condition). It also shows us how hard it is to up-titrate GDMT. Even with this intensive follow-up, barely a majority of patients reached goal doses – and this was before SGLT-2s were added to the mix. Furthermore, even with this level of attention, there was a 12% excess of adverse events.
One last point. If the first study might have been wrong owing it to being a single center study, this one might have been wrong since it was terminated early.
What should one take from this article? We should not conclude that patients should be started on 3-4 new meds prior to discharge. We should conclude that patients will do better if they are assigned to intensive follow-up with a heart failure team, staffed to provide this level of care. That is harder to do than writing a prescription. It will probably mean spending more money of patient care and selling fewer drugs.
Baseball factoid. Three player have hit home runs in 8 straight games: Ken Griffey, Jr., Mariners -- July 20-28, 1993; Don Mattingly, Yankees -- July 8-18, 1987; Dale Long, Pirates -- May 19-28, 1956.
In addition to the problems you discuss, a fundamental problem with the breast cancer screening study is that it only analyzes those subjects who actually developed breast cancer, not the entire screened population. As I commented elsewhere (Doximity):
“The conclusion in the abstract states, “Annual mammographic screening was associated with lower risk of late-stage cancer and better OS across clinical and demographic subgroups. Our study suggests benefit of annual screening for women 40 years and older.”
This is misleading, since the study analyzes data only for the subset of women in the screening population who actually developed and were diagnosed with breast cancer during the study duration. One would need to analyze data from the entire screened population to draw any conclusions as to whether there is an overall statistically or clinically significant benefit to screening and if so how it compares to the risks and costs of overdiagnosis.
If such a poorly designed study were actually accepted for publication, the limited conclusion actually supported by the study data should be modified to read as follows:
“Conclusion
Among the subset of subjects who developed and were diagnosed with breast cancer annual mammographic screening was associated with lower risk of late-stage cancer and better OS across clinical and demographic subgroups. Our study suggests benefit of annual screening for those women 40 years and older who actually develop breast cancer but does not assess the benefit, if any, of screening all women 40 years and older.”
In my view, the study authors, peer reviewers, and journal editor(s) all share the responsibility for adding such a misleading study conclusion to the literature on this important and highly controversial topic.
One thing I like about reading sensible medicine on a Sunday is it keeps my brain from atrophying with the Sunday blues. Funny, how only four years into retirement I still dread Mondays…