
When do you need a disease expert and when do you need a data expert?
Should you call a cardiologist or an statistician?

When do you need a disease expert and when do you need a data expert? I occasionally find a reader in these pages wondering why we didn’t ask a mental health expert or infectious expert to opine on some topic, which John, Adam and I wrote about. That’s largely because those topics are data-expert topics and not disease-expert topics. At the same time, there are important domains where we would seek expertise from our subspecialty friends. Which is which?
I hope this article can help.
To keep it interactive— lets start with a series of polls. In each scenario vote for who needs the disease expert.
From Psychiatry:
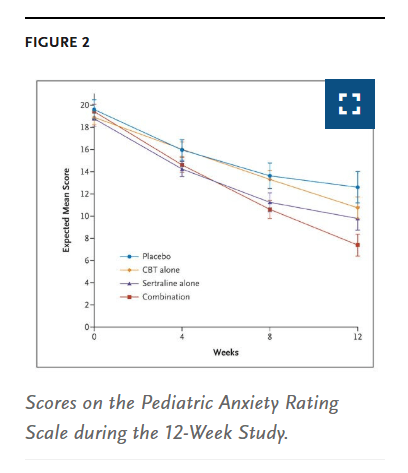
Patient 1 - a 7 year old kid says they feel anxious, and you are deciding whether or not they would benefit from starting an SSRI
Patient 2 - a 47 year old has stable bipolar disorder on Lithium for 15 years, but increasing urination
Patient 1 - A 57 year old had a stent placed two weeks ago for an occluded right coronary artery, and now presents with worsening shortness of breath— worse than before the procedure and it started suddenly.
Patient 2 - A 27 year old has LDL of 105 and normal weight, blood pressure and no other risk factors and is considering getting a coronary CT, lp(a) or starting a statin.
Patient 1 - A 57 year old has pancreas cancer and is on FOLFIRINOX. Feels weak after 3 months, and is wondering if he should go on hospice.
Patient 2 - A 57 year old woman (no symptoms) wondering if she should get a mammogram
Patient 1 - 42 year old wondering if he should get a fall covid booster?
Patient 2 - 48 year old with HIV on Biktarvy, with diarrhea that is not getting better, wondering if he needs more loperamide or should switch therapies?
It should be clear but deciding if a 7 year old should start on SSRIs, if a 27 year old needs a statin for cv risk, if a 57 year old should be screened for breast cancer, and if a 42 year old needs a annual respiratory virus shot— are data expert questions and not disease expert questions. What is the data that these interventions work? and are they worth it?
In contrast, how to manage lithium toxicity, the complications of a recent stent, whether a cancer therapy should be halted, or how to manage the side effects of HIV therapy —benefit from someone in the field.
The first category of questions have to do with whether, on average, for people in these situations, there is net benefit from a course of action. You can appeal to data, and if there is not great data, then one must appeal to one’s sense of risk and benefit. Do you think it is better or not to take a statin for 50 years without clear proof of benefit? Do you think a mammogram is worth it, given lack of all cause mortality benefit, and real risk of overdiagnosis, but possibility of reduction in cause specific mortality? No disease expert has any advantage over a thoughtful reader and thinker. In fact, they may be at disadvantage.
The latter category of questions are those that require modifying a planned course of action. There is, often, no gold standard evidence on when and how to modify, and seeking the guidance of someone who has rules of thumb may be of value. Even here, patient preference has a role, and even here, I would be careful not to assume the disease specific expert is correct. At the same time, it is nearly impossible to formulate an opinion in these situations based solely on reading. A data expert has no advantage.
A critic will say I am wrong. A child psychiatrist has a wealth of experience giving sertraline to 7 year olds, and knows when to give it and when not to give it. Furthermore, they know when to recommend CBT. What do you know?— they will shout. A data-expert can read this study, but has no idea how much anxiety is normal and when treatment is warranted.
Only the psychiatrist knows best, they will say. Oh really? 8 billion people are alive today, and some estimate that 120 billion people have ever lived. Of these 1.5% were and are 7 year olds— say a billion 7 year olds have ever existed. Researchers say 10% of kids may have anxiety. That might have been higher in times of war or famine. Let’s say maybe there have been 100 million 7 year olds with anxiety throughout human history. I believe that is probably a conservative estimate. What percentage have been seen by psychiatrists? 0.000000…1%.
And what do psychiatrists have to offer? In a short term study (inadequately short), there are tiny effect sizes from some course(s) of action, and a whopping placebo effect. What could a disease expert know about whether or not to give a child an SSRI based on their clinical experience when the effect sizes are microscopic, and no (good) effort has been made to see what are the long term consequences of starting a child on such a medication, and potentially taking it for 40 years (more on that below). Instead, in such a wicked learning environment the doctor may have learned superstitious behaviors. Akin to Skinner’s experiment giving rewards at random. A wicked learning environment is a situation where you cannot get ahead by experience— this is often the case in medicine when effect sizes are only visible from space.
Instead when it comes to a 7 year old that may or not be anxious, the dominant factor here is whether the parents believe this anxiety is something within normal limits, or something they will grow out of, or whether they believe 7 year olds should take psychiatric meds (I suspect most don’t agree with this). For 99.999999999999% of parents in human existence the solution was clear.
You may wonder why I have picked this extreme example. Why a 7 year old? I didn’t pick it! A JAMA expert did. Explained here.

A cardiologist knows more about lp(a) than you do— the critic will argue. That is true, but none of that has any bearing on whether or not a healthy 27 year old should take a statin for 50+ years. Someone who works in a movie theater knows more about where a soda was spilled last week—but that doesn’t help you decide if you want to the produce the Odyssey film.
I often see doctors on social media post videos saying “as a surgical oncologist, I know you should get a colonoscopy at 45…” That is as logical as saying “as a whitewater rafting guide, you should definitely drink a peaty scotch.” “as an interventional cardiologist, the right age to start zetia is in your twenties.” is akin to “as a circus performer, I always recommend 22 inch tires on your Tesla.”
Life is short, art is long, opportunity fleeting, experiment treacherous, judgment difficult. Knowing when you need a disease and data expert is knowing when you need experience and when you need experiment— judging which is which is difficult. On SM, we consider these matters carefully.