
"It's hopeless," the prospect of reforming cancer trials
A colleague doesn't pull punches

Recently, I had dinner with a friend and colleague visiting San Francisco for the SWOG (Southwest oncology group) conference. SWOG is a cooperative group-- nominally a collection of academic doctors who are supposed to run trials as a counterweight to pharma; guided by doing what is best for patients not profits. My colleague attended these sessions dutifully.
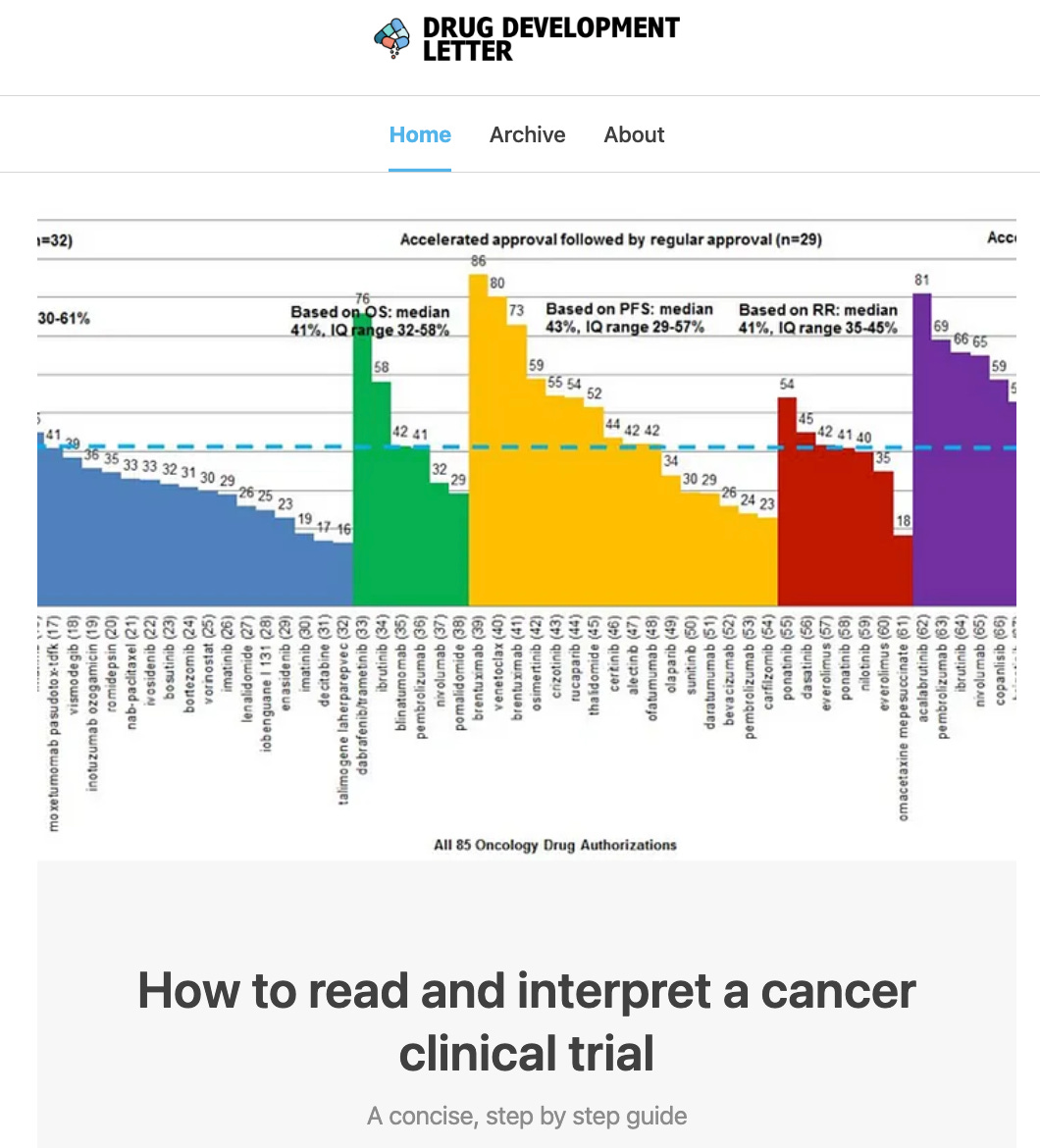
To understand our dialog here are some facts you need to know. The average cancer drug improves survival 2 months. New drugs often cost 200000 per year and there is no correlation between benefit and price.

Figure from: Miljkovic, Tuia, Olivier, Prasad JAMA IM
Some new drugs-- like CAR T in myeloma-- cost 400000 per dose and cure no one. Many cancer trials that bring these products to market have serious deficiencies, which my research (and Plenary Session podcast) has described over the last decade. My colleague is a fan of this work, sees the same problems I do, and tries to fix them in his way. He attended the conference and spoke as often as possible.
“It's hopeless.” He told me over drinks, “I am literally the only person in the room saying maybe we should measure overall survival and not just pathCR or EFS or MRD. Its just hopeless. ” he told me.
The most common errors in cancer trials work to ensure that the data are not actually applicable to average Americans. Over the last 10 years, we have done work showing many trials lack control arms, use inferior controls, measure unreliable endpoints, have the inappropriate use of crossover, poor post protocol care or improper drug dosing. After having written on these topics for a decade, I wrote a book explaining these challenges called Malignant. And a short primer for the Drug Development Letter if you are interested.
“No one there has read your book, obviously,” my colleague went on, “but worse, even if they had, they wouldn’t give a shit. You can't stop the train. Pharma controls the entire narrative. The people chairing the sessions are the ones chairing the pharma trials. They are just thinking about their next consulting gig, while I waste my breath. It's hopeless.”
“What about the next generation?” I challenged him, “They are better”
“Yeah right.” He countered, “Not only are they mostly unaware of these issues, they are focused on their own IITs (investigation initiated trials) and industry trials and ad boards. And to top it off, it is all wellness and work life balance with them. They leave clinic at 12:01 and reschedule the patients are in the lobby.”
“Well, what's your solution?” I asked
“You have to come personally next year,” he said.
“What am I going to do?”
“You are more persuasive than me.”
“You think I will persuade everyone?”
“No, of course not, I just want to see you face when they talk.”
That's how the conversation ended. Not with a bang, but with a whimper.
Was my colleague too cynical? A product of not enough work-life balance? Or was he stating an uncomfortable truth? I wondered in the days that followed.
What do you think?
““What about the next generation?” I challenged him, “They are better””
The generation that eagerly thought masks could stop a virus, made elaborately choreographed Tik Tok dances to show how hard they were working in the hospital and advocated for kids to not go to school?
That generation?
Here’s my glimmer of optimism: all this corruption used to be known only to a small group of dedicated clinicians, like yourself. Now thanks to Covid related lies/corruption, millions and millions more people understand how broken the system is. We are much closer to reform than ever before - thanks to the astonishing loss of trust people have experienced with medicine!
More here, with Solzhenitsyn’s perspective as a useful starting point (yes, from the gulag… nobody ever said this was going to be easy):
https://gaty.substack.com/p/2023-preview-the-end-of-medicine